
Commentary
Empowering Voices: The role of trustworthy adults in youth Sex Ed
Outside of family, our youth’s primary resource for sexual education is school, and we know there are limitations on what schools can provide
By Brittinae Phillips | LOS ANGELES -Through leading and delivering education programs for Planned Parenthood Los Angeles’s Black Health Initiative for the past four years, I have had hundreds of in-person conversations with thousands of youth and young adults about sexual health, sexuality, and relationship values.
What I’ve learned over and over from these experiences is that vast misinformation, confusion, and stigma about sexuality and sexual health remain pervasive in the minds of our young people, and the resources they have on these topics simply aren’t enough.
With content from the internet perpetually at our fingertips, it’s easy to have the misperception that today’s emerging adults are savvier when it comes to sexual health and education. But in my work, I see wide gaps in knowledge and understanding. In my sessions, I hear the same questions about basic body anatomy, the difference between sexual orientation and gender identity, and, what’s more, bewilderment about hurtful sexual stereotypes, particularly those aimed at Black men and women.
It’s important to remember that outside of family, our youth’s primary resource for sexual education is school, and we know there are limitations on what schools can provide. Consider that as of September 2023, only 38 states, along with the District of Columbia, mandate sex or HIV education. Within this group, a mere 20 states insist on including contraception education, and just 18 of these states mandate that the information provided be medically accurate.
Even here in California, health advocates report that the implementation of existing laws, limited funding to support training for educators, and the lack of broad health education requirements all continue to create barriers to sex education for young people in the state.
For youth who may have questions about LGBTQ+ topics, resources are even more scant. Only 10 states and DC require inclusive content about sexual orientation, and four states require only negative information to be provided on homosexuality and a positive emphasis on heterosexuality. California is unfortunately not immune to gaps in this area either.
A 2022 report developed by Equality California revealed that only 52% of districts have adopted LGBTQAI+ inclusive social science textbooks at the high school level. Advocates also report a significant rise in opposition at the local school board level to implement sex education, particularly to LGBTQAI+-inclusive or historically accurate content.
Our teachers are doing all they can to give their students accurate knowledge and helpful tools. But we must acknowledge that this patchwork of requirements and varying standards means that a comprehensive understanding of sex education eludes many young people, leading to a concerning lack of knowledge.
The exclusion of LGBTQ+ topics not only deprives students of vital health information but also misses the opportunity to answer questions from students of any orientation that could help foster compassion and understanding, leaving intact all-too often discriminatory environments for young people who identify as LGBTQ+.
For many, I know this feels both familiar and “bigger than just me.” But I encourage readers to remember how they felt as young people, the questions they had, and the confusion they may have endured. Are we content to hope that today’s young adults just figure it out? My experience shows me they are looking for more than that.
I can say with certainty our young people want to talk – they are looking for trustworthy adults to ask questions and express their concerns. Whether as a parent, family member or friend, I know it can be challenging to broach these conversations. Starting them can feel awkward, and young people may posture they’re “in the know,” but they need to discuss these topics. Below are some of the principles I follow in my classes to spark these conversations.
- Check your surprise. Most of the anonymous questions I receive from young adults are about anatomy and basic human biology. Let them know it’s okay to ask these questions – they need to understand their bodies to care for themselves.
- Words do matter. There are a lot of terms available today that people can use to describe their sexual orientation or gender identity. It’s important for adults to understand these terms so that they can have better conversations with youth.
- Talk about consent. Consent is a critically important topic to learn about – it is everyone’s responsibility to learn how to both say no to situations that aren’t right for them and listen when someone says no, and act appropriately. This includes asking for a yes, rather than waiting for a no.
- It’s essential to really listen. If they feel like you are really listening, they will feel better
about talking with you. Listening without judgment will help young adults figure out what’s best for them and live by those values.
- Be a role model. Young adults want to talk about these topics and seek support and guidance. You can be honest about information while still underscoring the benefits of healthy behaviors and decisions.
- You don’t have to have all the answers. If you can’t answer a question, work together to find the answer. Giving wrong information or not answering the question does not help someone make healthy choices.
We can overcome inaccurate information and damaging stereotypes through more of what my team and I do daily – giving young people a safe place to have honest, attentive conversations. Even more reassuring is that we all have the opportunity and ability to make a positive difference in a young person’s life by intentionally making space for them to address sensitive topics. I hope to inspire proactive action.
To get information or resources, please visit: https://www.plannedparenthood.org/learn/parents.
******************************************************************************************

Brittinae Phillips, Sr. Education Manager for Planned Parenthood Los Angeles’s Black Health Initiative manages community outreach and education for parents, college students, and youth in diverse communities throughout the county

Opinions
Gay for pay: Andy Lee and the changing face of content creation
Are the lines between identity and performance more fluid than we’re ready to admit?
In today’s ever-fapping world, the intersection of sexual identity and content creation has become more complicated than ever. Irish content creator Andy Lee, cozily ranking in the top 0% of OnlyFans creators, with his furry physique and tatted up torso, is at the center of the conversation. A self-identifying hetero who rose to prominence during the Pandemic, Lee has amassed a girthy following of horny gays, likely because of the exclusive man-on-man content he has to offer. Yet, his success raises just as many eyebrows as it does trousers. Many question the authenticity of his content, sexual identity and whether or not straight men are overshadowing their openly gay peers.
Claiming to be straight only to then go pole-to-pole on camera, Lee is seen by a significant portion of the queer community to be guilty of queerbaiting (exploiting gay culture for profit). Others can’t help but wonder, is this slab of man-meat genuinely drawn to the physical (and perhaps emotional) experiences he has with men, despite identifying as a thorough(ly) bred breeder?
Lee’s OnlyFans career showcases the blurred, often contradictory nature of sexual identity. He enjoys sexual experiences with men but still identifies as straight, which challenges traditional labels like “gay” and “straight.” His content forces us to confront the nuanced lines of sexual identity, which are rarely ever clear-cut and often defy simple categorization.
The question of authenticity also hangs in the amyl nitrite-scented air. While Lee has said his career on OnlyFans has made him feel “wanted and loved” (and paid) by the gay community, many argue that his identity as a straight man undermines the emotional connection his audience thirsts for. Is his content less authentic due to its “no-homo” viewer discretion warning, or does his openness to explore other men’s bodies reflect the evolving, fluid nature of human sexuality?
This has led to several openly gay performers to claim that, well, “they’re taking our jobs.” They argue that by creating gay content for profit, straight men commodify gay experiences while avoiding the brunt of the stigma that accompanies being openly gay. But how valid is this criticism? In a consumer-driven adult content market, if people choose to engage with Lee’s content, are they unintentionally depriving the gay sex-working community?
And then there is the aspect of the gay gaze (did not stutter). Is it the allure of the forbidden nature of straight men giving into the carnal pleasures that another man has to offer? The taboo? The challenge? Or are they simply the proxy of the coach you had a crush on in high school, the hot trainer who you overheard has a girlfriend, or that college professor you once stood next to at the urinals only to find out for yourself just how extensive his curriculum was? For many, this particular brand of tension is a huge part of the turn-on.
This paradox is just one part of a broader cultural conversation about masculinity and sexual identity. Straight men in gay content can subvert traditional gender roles, while simultaneously reinforcing certain ideals of masculinity. In cases like Lee’s, when a straight man openly enjoys the physical pleasure of being with other men, it speaks to both the complexity and fluidity of sexual identity, and the inability of inflexible labels to accurately and respectfully encompass human desire.
Ultimately, the conversation around gay-for-pay creators like Andy Lee isn’t black and white, straight or gay. Although likely unintentional (let’s be real), these performers challenge existing ideas of identity, authenticity, and the commodification of desire. Whether Lee is queerbaiting, exploring his own sexuality, or just making stacks of cash, his presence in the adult content world invites folks to rethink how we define sexual identity today. Just something to think about next time you’re… enjoying content.
AJ Sloan is a writer, retired adult performer and clinical counseling graduate student. His work has been featured in Huffington Post and The Advocate and led his own weekly column for Fleshbot.
opinions
Why is it important for cities to become LGBTQ sanctuary cities?
This is not just a win, it is a small, but monumental stride toward progress, representation and protection

When a city passes the motion to make their city an LGBTQ sanctuary city, it means that city or state resources cannot be used to prosecute or punish LGBTQ people for seeking gender-affirming care, resources or government assistance.
As many of us know, there are three major levels of government: local, state and federal.
City motions set a precedent for the state, adding local representation on a small scale that hypothetically catches on and makes its way up the ladder to the state, then federal level.
Though the Trump administration holds a lot of power on a federal level, states, cities and municipalities hold power on a level that is easier for local communities to change and control. If cities across the state begin passing motions to become LGBTQ sanctuary cities, the state then has to consider passing the motion to become a sanctuary state. If the majority of states consider themselves sanctuary states, it pushes the change on a national, or federal, level.
At first glance, it seems like the move for a city to consider itself an LGBTQ sanctuary city is not a big deal because there is no financial flow in the motion and there are no special funds to be allocated. The only visible change is the new title the city gets to claim. However, passing motions in favor of LGBTQ rights, is crucial toward the longer and harder journey to attain rights on a national level. It is a far more nuanced issue than what it seems.
If that same logic were to hold up when it comes to statewide decisions, then it could become easy to dismantle progress made on any level.
The Advocate published an article in November when the City of Los Angeles unanimously passed the ordinance to become an LGBTQ sanctuary city. Passing the ordinance means that the city is now responsible for “shielding queer youth who travel to the city to receive gender-affirming care from prosecution, as well as preventing city resources from being used in immigration enforcement or assisting federal immigration officials.”
During the November 2024 election, Proposition 3 made it on the ballot and Californians had the choice of voting in favor or against the proposition that would only change the outdated language of the California state constitution, that until recently did not recognize same-sex or interracial marriages. To some, the change seemed meaningless, but on a statewide level, passing this proposition meant cementing the progress made on the protection of same-sex and interracial marriages. Though the proposition had no money flow in the matter, this important move signaled the support of the state in favor of LGBTQ rights on a state level.
While California is already a sanctuary state, it is also crucial to recognize protections and rights in individual cities. During these unprecedented and uncertain times in LGBTQ history, it is more crucial than ever to push for these changes.
When one city makes the move to become a sanctuary city, others follow and LGBTQ representation becomes more visible on a government level.
In November, shortly after Trump was elected as the 47th president of the United States, Los Angeles declared itself an LGBTQ sanctuary city.
Now, Long Beach has followed suit and has unanimously approved a resolution to make the city a transgender sanctuary city and officially recognize March 31 as Trans Day of Visibility.
There are a growing number of LGBTQ sanctuary cities across the nation. In California, the list of cities includes San Francisco, Sacramento, West Hollywood, Los Angeles and most recently, Long Beach.
Other cities, including Boston, Massachusetts; Olympia, Washington; Cambridge, Massachusetts and others across the nation have also recently declared their status in support of LGBTQ people.
This is not just a win – it is a small, but monumental stride toward progress, representation and protection. We need more cities to push motions to become sanctuaries for queer and transgender people as the current administration continues to use queer and trans people as political pawns in the chess game rigged for the alt-right.
Miscellaneous
Gay bar in California bans MAGA gear — but no other political expression — from its premises
MAGA is a terrorist threat to the LGBTQIA+ community
Do not let anyone bait you into a “both sides” argument on this topic. Trans people can confirm that we no longer live in a country where freedom of expression exists in the first place, so the point in and of itself is moot. Don’t waste your energy.
But especially don’t be shamed by those who imagine themselves to be more enlightened than you as they make the tired false equivalence that MAGA is just another political ideology that deserves the same freedom of expression as liberal points of view.
The owners of the Badlands Bar are keeping their patrons safe from terrorism. Yes, MAGA is a terrorist threat to the LGBTQ community. Oxford’s definition of terrorism is “the unlawful use of violence and intimidation, especially against civilians, in the pursuit of political aims.”
It’s too long a list for this article, so here’s a link to a running tally of the government’s actions against the LGBTQ community since Jan. 20.
It started, on Trump’s first day as president, with trans people being forcibly stripped of their very identity — and with it, all protections — under the law. This trend has continued, ominous drip after ominous drip of frequently illegal Executive Orders that dehumanize, disenfranchise and dismantle the basic rights and dignities of trans and queer Americans. If you’re following the Project 2025 playbook, as the federal government is, you’ll notice that ending marriage equality is quickly coming up on MAGAs To Do list.
All of that—the bullying, the emotional and psychological abuse, the stripping of rights, the (eventual, inevitable) tearing apart of families—is violence, by definition. The anxiety you feel every day as an LGBTQ American? That’s intimidation. And that is why living under MAGA as an LGBTQ person means living in a terrorist state.
Perhaps the idea that MAGA perpetrates outright terrorism seems dramatic, especially for those who remember 9/11 and maybe we don’t need to add more drama to this historical moment.
Then let’s consider the terrorism of words and ideas.
Stochastic terrorism, is a particularly nasty form of political expression, where those with cultural power spout hostile rhetoric about a group, creating a culture of hate that inevitably — but not directly — results in violence. When we talk about haters becoming emboldened by Trump’s rhetoric, this is the dangerous potential that absolutely does become reality.
The insidious part of stochastic terrorism is that there’s plausible deniability on the part of the instigators. Truly, who do we blame for the murder of Lauri Carleton in Lake Arrowhead, CA?
Do we blame the individual who shot her after he screamed epithets about the Pride flag she flew in front of her store? Or do we blame the talking heads and podcast hosts who were then spending untold airtime equating LGBTQ people with pedophilia and grooming? Or do we blame the governors who sought to ban the flying of Pride flags in public, for turning them — and all of us who fly them — into high-profile lightning rods for hate? Who should be charged in a court of law for this hateful crime?
If any comparison to terrorism still seems too far-fetched to you, even for MAGA, then let’s consider the term “gang.”
Flip all the racist rhetoric you’ve passively absorbed about the kinds of people most likely to be in a gang, and consider Donald Trump, the current Republican Party, and MAGAs specifically as you read the following definitions of what a gang is.
According to the Department of Justice:
- Gangs adopt a group identity in order to create an atmosphere of fear or intimidation.
- Gangs are typically organized upon racial, ethnic, or political lines and employ common names, slogans, symbols, hand signs, or style of clothing.
- The gang’s primary purpose is to engage in the use of violence or intimidation to enhance or preserve its power, reputation, or economic resources.
If we hold MAGA to the DOJ’s gang standards it so easily fits into, perhaps we can more easily hold that most businesses explicitly bar gang symbols from their premises, often as an easily-enforcible safety measure, and consider the Badlands Bar owners’ actions in that context.
But if you’re still suspicious of any of this rhetoric, then all that’s left is to consider the reality of MAGAs actions, which owners of LGBTQ bars around the country experience on a regular basis.
On Feb. 22 at Scorpio, in Charlotte, NC: an exception made to a “no political affiliations of any kind” dress code, devolved into the individual making transphobic remarks at the entertainers during the drag show. He refused to leave when asked and became aggressive toward security, resulting in police intervention.
On March 14 at the Chatterbox Jazz Lounge in Indiana, MAGA hat-wearing patrons aggressively misgendered and harassed a bartender and were ejected. The video of the altercation went viral; the owner reports his bar has since received several threats of arson and bodily harm.
Four days after the video of that incident went viral, the Chatterbox Tavern in Tennessee received threatening emails and phone calls.
These incidents were flashpoints that reported, often by MAGAs claiming victimhood. Untold incidents go unreported due to intimidation or uninvestigated due to bias. According to GLAAD’s 2022-24 ALERT Desk Report, over 1,850 anti-LGBTQ incidents were reported across all 50 U.S. states. That’s more than 600 acts of vandalism, bomb and mass shooting threats, assaults, and cases of arson per year — nearly two per day. These incidents have resulted in at least 161 injuries and 21 deaths. The perpetrators — when apprehended or known — wore MAGA gear, screamed MAGA slogans, had shared MAGA rhetoric online, or were members of MAGA-associated groups like the Proud Boys, Q-Anon, Three Percenters, Libs of TikTok and Moms for Liberty.
If after all of this — and the rest yet to come — you still believe that MAGA simply represents an opinion about a stance on taxes, individual liberties and the size of government, then this author will be the bigger person and acknowledge your identity as part of America’s inherent Diversity, wholeheartedly Include you as an Equal in this vast multiplicity to which we belong called America.
And then ask you, if it’s all directly equivalent: when will MAGA do the same for LGBTQ people?
Of course you are free to wear your red hat and shirt wherever you please — your gang runs this place, after all. You’ll even be pardoned for violence you commit, like the Jan. 6 terrorists and your poster boy Kyle Rittenhouse. Don’t fret.
But don’t expect us not to protect our own just because we’re a bunch of queers.
The author of this Op-Ed wishes to remain anonymous for safety reasons, given the nature of the issues discussed. Citations are linked to GLAAD’s expert resources, but this Op-Ed was not written by anyone affiliated with the organization.
Community Perspectives
Have our gay gyms gotten a little too steamy?
As gyms shift their focus to serve a broader, younger, more mainstream clientele, the future remains unclear
One undeniable truth still stands: public sex acts of any kind are illegal, as in, against the law.
Another day, another endorphin-boosting pump at the gym.
Next stop: the steam room.
My circulation and lactic acid levels will thank me later. After a quick shower, I approach the steam room door and, to my surprise, I see a notice taped to it:
STEAM ROOM RULES
Guests entering must be dressed appropriately.
Workout shorts, swim attire, or towel ARE REQUIRED at all times.
Camera use is allowed ONLY within the STEAM ROOM AREA.
Initially, I was taken aback.
In an environment meant to offer a moment of relaxation before diving back into the chaos of the city, the last thing anyone needs is a dose of CCTV surveillance. My shock was brief, though, as I quickly realized why the gym had taken such a drastic step.
This issue isn’t unique to New York City or David Barton’s Gym U. After several closures and re-openings of their steam room, Crunch WeHo — another predominantly gay gym — has indefinitely closed its men’s steam room. I also learned that a Crunch location in Brooklyn has followed suit. I imagine both gyms now display similar notices warning that ‘inappropriate behavior will not be tolerated.’
As anyone who’s frequented a gym’s steam room in any major city knows, these spaces are no strangers to cruising. This isn’t a new phenomenon. For decades, gyms – and their locker rooms and amenities — have served as ground zero for gay cruising. If this surprises you, pick your jaw up off the floor and Google the meaning behind the village people’s
Young Men’s Christian Association. You might feel a little awkward the next time it’s sung en masse at a sports game or (eye roll) an inauguration.
Many see cruising as part of a shared gay culture at these unofficially gay fitness clubs. However, the growing number of complaints to gym staff about these post-pump antics suggests otherwise. This raises the question: has the ‘inappropriate’ behavior in these spaces become so prevalent that closures and Orwellian surveillance are now the only solutions?
Years ago, same-sex sex was a criminal act and treated as such. Back then, sex became a form of protest for many gay men and others in the LGBTQ+ community. It was a way of saying, ‘We exist, we have the right to exist and we have the same right to get off as anyone else.’
Since then, both the LGBTQ+ community and the politics surrounding it have evolved. With more queer people adopting what many consider a heteronormative or family-oriented lifestyle, and with the rise of sex positivity, can we still view sex as a form of protest? On the other side of the three dollar bill, are those who are getting down in the dank dark of our steam rooms seeing this action as a way of preserving a tradition that they hold near, dear and queer?
This situation is a bit more layered than a simple ‘then and now’ generational shift. Over the decades, certain fitness centers in cities like New York, Los Angeles and Chicago have been recognized as gay spaces, with a loyal, predominantly gay clientele. However, now these gyms are distancing themselves from their LGBTQ+ identity — sometimes quite literally shedding their pride flags.
Now, they’re offering student discounts not to the City Universities of New York, but exclusively to NYU and PACE — targeting a younger, straighter and more affluent clientele. So, when ’23-year-old finance bro Bobby’ walks into the steam room to find two men in the middle of a vigorous forearm workout… Sorry Bobby.
It’s the ultimate risk that comes with sneaking in that last “spot” off the gym floor. Many folks who don’t partake turn a blind eye – or even offer a blasé wink when they walk into the steam room. Then there are those who would prefer a steam room where people’s hands remain in sight while their other bits do not. In today’s tense political climate, is it ending up on a list forbidding you to be within 500 feet of schools?
Ultimately, the steam room – a once cherished space with a sense of freedom and unspoken connection as palpable as its wafting clouds of moisture – has found itself to be a microcosm of the broader tensions both within the LGBTQ+ community and society. As gyms shift their focus to serve a broader, younger, more mainstream clientele, the future of steam rooms remains, well, unclear.
AJ Sloan is a writer, retired adult performer, and clinical counseling graduate student. His work has been featured in Huffington Post and The Advocate and led his own weekly column for Fleshbot.
Community Perspectives
Why does Hollywood still struggle with trans representation on screen?
People outside the trans community can resist the unprecedented injustices by keeping trans people visible, telling our stories in ways that expose the lunacy of our nation’s politics and casting trans actors in roles that have nothing to do with gender.
Hollywood and anyone watching the ‘For Your Consideration’ film and TV series, should agree it’s time to lay this issue to rest.
Star of Beyond the Gates, Karla Mosley, told People she will not be playing another transgender role, calling it “truly inappropriate.” Mosley has always been a strong advocate on this issue of transgender representation on film and TV.
I’m personally sick of this debate I’ve embodied for a decade as a transgender actor. It needs to end – and yet the talking points persist.
I was the first out trans actor in Daytime television as the actually trans counterpart to Mosely’s transgender character on The Bold and The Beautiful. Ten years ago, Hollywood insisted, ‘actors should be able to play anything.’ Our response?
‘Then why weren’t trans actors cast in anything—even our own stories? Why was playing trans Oscar-worthy for cis actors while trans actors struggled to book speaking roles?’
There are always exceptions such as Jazzmun Crayton and Alexandra Billings – who deserve Lifetime Achievement Awards. But those divas each represent a dozen equally talented artists who couldn’t even get an audition.
Denying Hollywood’s past transphobia disrespects the transformation many Hollywood powerbrokers underwent to measurably level the playing field. And I was there – our fight in 2015 was against rampant transphobic employment discrimination.
Once we finally gained access and visibility, we wanted better representation. Watch the Netflix documentary Disclosure, for decades of psychotic killers and punchlines that trapped trans people in life offscreen. We’ve got receipts!
In the now quaint era of diverse entertainment (2015-2024, R.I.P.), we collaborated with cis executives who, even as they included us, still clung to their own idea of who we are.
But we made progress.
With a dozen others, I consulted behind the scenes on countless tv shows and films. We enriched storytelling with accuracy, vivid detail, and dialogue that leapt off the page.
Audiences had never seen anything like it.
Most creatives and production teams embraced this project; many had trans kids and wanted to create an inclusive world for them. Those who resisted lamented that the Hollywood system they dominated — founded in exclusion, maintained by abuse — had to change at all. As you consider my proposal, ask yourself: is that really the side you really want to take?
Trans actors agree — we can play any role!
First we must be called in to audition, then we must meet approval by approximately five levels of producers and executives to light up your screen. Too often, we run into Old Hollywood gatekeepers, or outright transphobia. The solution? See us for more roles—all roles. Flood the gates.
The urgency for showrunners and filmmakers to take this next step has never been greater. The frontman of this increasingly fascistic government now controls the Kennedy Center and mandated that the National Endowment for the Arts focus on America’s semi-quincentennial — while explicitly excluding diversity, drag, and trans stories.
Filmmakers and executives, now is not the time to pre-comply. Now is the time to uphold freedom of expression on any platform that will still allow it. Trans people embody freedom of expression! When a repressive government insists on rigid gender binaries, expand what it means to be a man or a woman. In a country determined to erase trans people from public life, star us in your stories, let us shine.
Commentary
Real Housewives, The Traitors, and Denise Richards Recaps…Oh my!
Your weekly reality TV tea from Drag Maven Norma Lee!

‘And still, I rise.’ If you’ve been using this quote nonstop this week, you have also been obsessed with the instantly iconic third and final part of The Real Housewives of Potomac reunion. The final chapter in season 9 of RHOP really had it all.
No joke, I’ve watched it three times this week. In case you missed it, QVC queen Stacey Rusch got dragged by the women, the production and the man she allegedly paid to play her boyfriend on TV. This man not only said Rusch hired him to be her boyfriend on TV, but she also still owes him money for it. Rusch did not believe it until production brought out the raw footage and even then she kept it calm, cool and collected. Either way, she earned her spot in a second season. Meanwhile, between that bombshell and the ‘oh-so-staged’ Karen Huger video, the other ladies were reading and roasting the house down. Then they went in on Huger and everyone spilled the tea about her day drinking around the D.C area.
What a great finale! Also, Mia wasn’t there because she left in a huff last episode, which leads to the question: do we still need Mia Thornton for season 10?
Talk about a show to put you to sleep. Let’s jump over to our home franchise of Real Housewives of Beverly Hills. Why am I so bored this season? Even this lively episode of Sutton’s fashion show gave meh the whole time. The only thing worth mentioning from an hour-long episode is that Kyle Richards was hurt after photos surfaced of her estranged – and hot – hubby Mauricio Umansky, kissing another woman at the airport.
She had a whole meltdown about it as if she hasn’t been flaunting her late-in-life lesbian relationship all over TV, social media and the paparazzi. Richards, give it a rest and come out. Do your part to make this boring show somehow interesting. I do love that Garcelle Beauvais is determined to out her on TV, which seems fair after Richard’s involvement in the whole Denise-Brandi drama a few years back.
Speaking of Denise Richards, I gave her new spin-off Denise Richards & Her Wild Things a shot. It’s random and not really worth watching. Almost all the Housewives of Beverly Hills past and present make cameos throughout the season, which feels a tad desperate. She did somehow manage to bring up again how hung her hot husband is in the first episode, but is that enough to keep the gay audience? Doubtful.
Now a reality show that totally delivered this week was the finale of The Traitors on Peacock.
Spoilers ahead!
In the final episode of the Emmy-winning competition, we saw traitor Danielle finally go home, sent packing by her Big Brother fr-enemy Britney. Now Britney is the only traitor left in the finale and the faithful must either banish her before it’s too late or lose all the prize money. Luckily, cutie Dylan Efron puts the pieces together and sways the rest of the castle to vote out Britney. Then the four remaining players decide to split the winning and the game is ended. The best gamers in the world competed and yet, Traitors was won by a royal, a bachelorette, a real housewife, and a nepo celeb. That’s TV gold, folks.
Opinions
Newsom is playing right into the far-right’s playbook
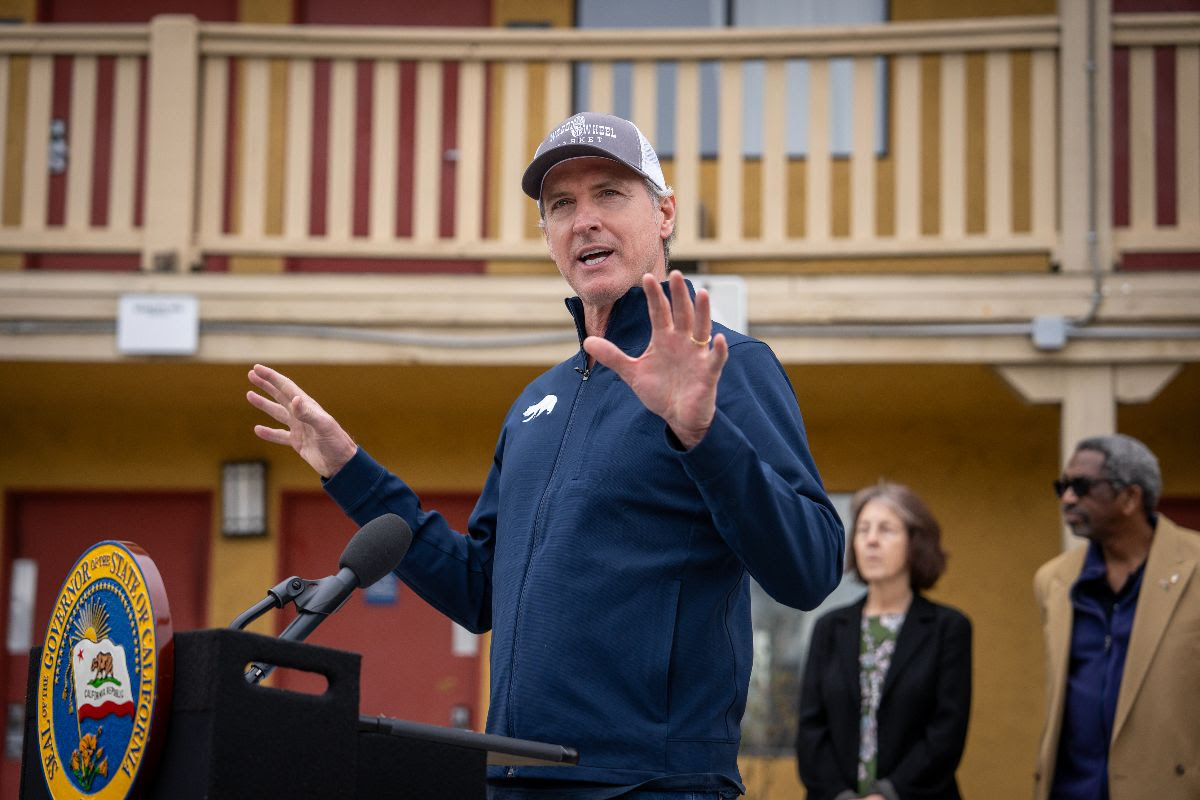
A democratic political leader who built a reputation on standing ten toes down for the LGBTQ+ community and being the political rebel that Trump has vowed to take down, has seemingly joined the dark side.
Late last month, California Governor Gavin Newsom released the first episode of his new podcast titled, “This is Gavin Newsom.” This week, he released the second episode featuring his first guest, Charlie Kirk.
Kirk is a 31-year old conservative “activist” and founder of the right-wing student organization Turning Point USA. The episode gained media attention because Governor Newsom has always stood behind LGBTQ+ rights and has always been a vocal advocate for LGBTQ+ protections on the local, state and federal level. He has gained political support and built an entire career on the backs of LGBTQ+ Californians and what he seems to be forgetting right now, is that LGBTQ+ includes the transgender community.
The trans community is one of the most politically vulnerable communities who are constantly undergoing heavy, hateful and misinformed political attacks.
It came as a shock to hear Gov. Newsom speak on this issue and sound just like a far-right republican who’s been against trans Americans since the very beginning. During his two terms, he has advanced LGBTQ+ protections and fundamental rights by signing laws that cement rights.
In contrast to all this progress he’s advocated for, he took the stance against allowing trans athletes to participate in women’s sports – a hard betrayal to the community that was counting on him more than ever. The current administration is hostile and extreme in their attempts to erase gender nonconforming and trans people and a politician like Newsom, was a diamond in the rough when it came to LGBTQ+ issues.
“I revere sports and so the issue of fairness is completely legit,” said Newsom in his podcast episode. He was referring to his view on fairness regarding trans women and young girls in women’s sports competitions.
Many organizations and leaders across California have responded to his views of trans women competing in women’s sports.
CEO and founder of TransLatin@ Coalition responded with outrage and disappointment.
“The TransLatin@ Coalition is extremely disappointed and enraged about the remarks made by Governor Gavin Newsom on his podcast on the issue of trans youth participating in sports,” said Salcedo in an Instagram post.
The Coalition called out his message about trans athletes by mentioning his need for support from conservatives for his potential bid for presidency.
“This is probably a stunt by our governor to align with conservatives to set himself up for the presidency, but he is fooling himself if he thinks this is the route.”
Around the same time, the Los Angeles LGBT Center issued a statement condemning his exclusionary message about trans athletes.
“Newsom is parroting the same Republican talking points used to marginalize and erase trans people,”said Joe Hollendoner, CEO of the LA LGBT Center. “This is an appalling betrayal from someone who once positioned himself as a champion of equality and demonstrated such strong leadership on behalf of LGBTQ+ people during the first Trump administration.”
What Newsom and the alt-right extremists who use the fairness argument in response to trans athletes need to understand, is that trans rights are not up for debate.
Athletes, trans or not, should be able to compete freely in sports under the First amendment.
If it were a matter of fairness, they would also consider it unfair to have trans men compete in the male divisions of sports, yet they are not mentioned in any of the legislation aimed at supposedly making sports more fair.
What Newsom is parroting, aligns with one of Trump’s recently signed executive orders which is titled ‘Keeping Men Out of Women’s Sports.’
The deeply disturbing and entirely misinformed perspective outlined in this executive order is sold to Americans as a form of protection and privacy for athletes, but in fact guarantees the opposite. Athletes will have to continuously undergo unfair and accusatory situations with no one to defend their position, whether they are trans or actually cisgender. This executive order and by extension, the position now shared by Newsom, actually endanger athletes who are cisgender, by relaxing privacy policies that would allow for investigation and prosecution of athletes who are accused of being trans, such as the Utah teen who was accused of being trans and put in danger by the public statement made by a Utah state school board member named Natalie Cline.
Last year, a more prominent example made headlines across the country regarding Imane Khelif, an Olympic boxer who was attacked with hate speech, conspiracies and accusations regarding her gender. She was exposed to bullying and hate by people who questioned her gender, completely ignoring the fact that she was born a female and has competed as a female for many years.
After her first win in the Paris Olympics where she won the fight against her opponent in 46 seconds, frequent critics of transgender rights, including Elon Musk and J.K. Rowling quickly took the opportunity to weigh in.
The mention of Trump’s lapdog, Musk, sickens me but also brings us full-circle to who is funding this anti-trans machine from the very root of the problem. He is not only Trump’s lapdog, but he’s also a multi-billionaire with too much time on his hands and nothing diplomatic or important to say about trans people. Let us not forget that his villain origin story began when ex-wife and baby mama was rumored to be dating infamous trans WikiLeak-er Chelsea Manning after breaking up with Musk.
Since Trump’s inauguration, four other executive orders have been signed to target trans people and the institutions that support gender-affirming care and provide resources. The unfair and continued attacks on two-spirit, trans, gender nonconforming and intersex people, will not stop us from existing, but it will make it harder for us all to co-exist and thrive in a nation that is sold to the rest of the world as a free country.
Opinions
Trump’s allegiance to Putin is anti-American
Why have evangelicals forsaken their God for a fraudulent ‘savior’ who acts more like Satan in disguise?

Wake up. We’re slowly slip-sliding into a Russian-orchestrated coup.
This goes way beyond the jokey rumors that Russian dictator Vladimir Putin is blackmailing Donald Trump with a secret, compromising ‘pee tape.’ Consider how the U.S. voted in the United Nations with Russia, China and Iran against American supposed ally, Ukraine. Now there’s the shocking Oval Office ambush of Ukrainian President Volodymyr Zelensky by Trump and JD Vance.
As a smirking gaslit affront to Republicans, Trump is performing his excessive allegiance to Putin under the recently installed portrait of former Republican icon, President Ronald Reagan. Once upon a time, Republicans ascribed the fall of the totalitarian Soviet Union to Reagan’s strong, moral, anti-Communist principles.
“Let us be aware that while they preach the supremacy of the State, declare its omnipotence over individual man, and predict its eventual domination of all peoples on the earth, they are the focus of evil in the modern world,” Reagan exclaimed at the 1983 National Association of Evangelicals Convention in Orlando, Florida. He warned against ignoring “the facts of history and the aggressive impulses of an evil empire…thereby remov[ing] yourself from the struggle between right and wrong and good and evil.”
Where are the Republicans who cheered Reagan’s ‘evil empire’ speech now? Why do Republicans plug their ears when historians say Putin wants to restore the glory of the Soviet empire – by any means necessary?
Why do Republicans ignore the fact that former KGB agent Vladimir Putin is a communist.
By the way – where are all the Charlton Heston-loving evangelicals who watched him as Moses and cheered when he shouted from atop Mount Sinai, “Thou shalt have no other gods before me” – the first of God’s Ten Commandments. Look at that garish Golden Calf! It’s something charlatan Trump would feature in his NYC apartment or sell for crypto online.
Why have evangelicals forsaken their God for a fraudulent ‘savior’ who acts more like Satan in disguise?
I confess that I’ve been pissed off at evangelicals since rabidly anti-gay Rev. Jerry Falwell said AIDS was “God’s punishment for homosexuality.” Pastor Peter J. Peters wrote in 1992, “The Death Penalty for Homosexuals is prescribed in the Bible.” Now, Christian Nationals and their allies Trump & Putin make self-determined exceptions to the Ten Commandments while mouthing morality.
Nazi-loving Afrikaner Elon Musk’s unbridled enforcement of Project 2025 is not just about eradicating DEI but also about erasing us. Meanwhile, Democrats have been twisting in the wind trying to find a ‘message’ that will woo workers who believed Trump’s ‘populism.’ Pundits are advising the Democratic Party to stop talking about ‘identities’ and focus on ‘issues’ – with some progressives throwing trans folks under the bus to win votes instead of vigorously standing up for the values of fairness and equality.
Remember when Republicans were vehemently against government telling individuals what they can and cannot do and Democrats extolled the right to Freedom of Expression? Now, ‘identity’ is a slur.
Ask Black women if their race doesn’t impact their access to healthcare. Ask same sex couples if they fear placing a photo of their loved ones on their work desk might get them fired. Ask fundraisers and pollsters and nonprofit organizers if ‘identity’ demographics matter when voting on issues.
But none of this will matter if we don’t actively intervene to stop Trump’s Putin coup. Last week, former Fox Weekend co-host and current U.S. Secretary of Defense Pete Hegseth ordered the U.S. Cyber Command to halt “all planning against Russia,” according to a Feb. 28 report in the cybersecurity publication The Record.
The Recorded Future story reported how Russian state-backed hackers compromised SolarWinds Inc.’s systems and its Orion network management platform in 2023, distributing malware “to thousands of enterprises and government organizations” with “numerous other cyberattacks” discovered later.
“If Hegseth’s order only applies to the armed service members focused on Russia, it will reportedly affect several hundred cybersecurity experts,” though “several thousand personnel could be affected if the guidance also encompasses other teams,” The Report says. “Those other teams focus on tasks such as intelligence analysis and capabilities development.”
“How much more proof do we need that this administration is completely compromised?” Brian Krebs, a cybercrime and security investigative journalist, wrote on infosec.exchange. “There is zero reason for the US to relax any offensive digital actions against Russia. If anything, we should be applying more.”
This is hard. How close we thought we’d come to full equality with Obama, Biden, Hillary and Kamala – only to find, like the Paul Simon song says, “the nearer your destination/The more you’re slip sliding away.”
But we can’t give up. Rather, let’s take inspiration from the “Eyes on the Prize” series: “We Who Believe in Freedom Cannot Rest.”
Conclusion: America has switched sides in the Ukraine-Russian war. Up till now, we supported Ukraine’s existential fight for democracy, knowing they are on the frontlines for the free world.
I want to live & die knowing I fought for freedom.
Opinions
Shame On Hollywood For Being Silent Towards LGBTQ Issues At the Oscars
Everyone at the Oscars, but especially everyone involved in Emilia Peréz, had every reason — every responsibility — to say something.

For years, I’ve warned that when the government comes for trans people, they come for everyone. I’ve repeated how the relentless attacks on trans rights aren’t just about further marginalizing my community — they’re test runs for eroding everyone’s rights.
If lawmakers can strip a small, vulnerable group of their humanity — helped by a divided LGBTQ+ community and amplified by the media — they’ll also target other divided communities. In many instances, that’s how power works. That’s how oppression takes root and spreads. Another example of this issue is Roe v Wade — which is about what people do with their own bodies.
And then came the 2025 Oscars and Hollywood proved my point.
What some might call the Super Bowl for performative allyship, not one winner acknowledged the unprecedented anti-trans rhetoric and legislation that is fueling democracy’s collapse. Everyone at the Oscars, but especially everyone involved in Emilia Peréz, had every reason — every responsibility — to say something. This does affect us all.
As a professional trans media trainer, I can see how the PR agents and managers decided to downplay Karla Sofía Gascón’s existence entirely, even as she made history with her nomination as an out trans actress. Given the real harm of her comments, I almost understand it.
Almost. But not this year.
This is the first year a U.S. president — on his first day — declared trans and intersex people nonexistent. This is the first year the federal government vowed to defund hospitals if families, under the private, expert, care of specialist doctors, medically treat their trans children. This is the first year a trans child isn’t legally allowed to play T-ball. The first year trans North Americans are forced to carry passports that endanger us. The first year states re-write civil rights laws making anti-trans discrimination not just legal, but endorsed.
The machinery of government has moved in lockstep to make it clear: trans people are not wanted, protected, or safe.
If they are unhinged and ignorant enough to spend all those resources attacking .7 percent of the population — half of whom were literally ‘sissies’ on the playground — some part of you knows they won’t think twice to attack you.
This was the year to rise above past mistakes — to let a sincere apology start a new chapter, not perpetually punish for lack of purity. This was the year that ignoring trans people when you had the most-watched opportunity to rally for us — played into the hands of history’s villains and confirmed how they should continue mistreating trans people.
We need to see that clearly so we can change how we operate and save ourselves. You need to start believing the trans advocates like Erin in the Morning, Chase Strangio, and TransLash Media.
Maybe celebrities will want to speak out at future Oscars when their own basic rights are threatened.
Or, maybe then they’ll understand how staying silent on trans people was actually them cutting their own mic.
This is the Diversity, Equity and Inclusion work the government wants erased, so every word is resistance.
Scott Turner Schofield is an actor, writer, producer, speaker, and trans activist who transitioned 25 years ago and followed their calling to become an advocate. Ten years ago, Schofield became the first out trans actor in daytime television and made it his mission to build a trans-inclusive Hollywood. They’ve had a front row seat in the transgender representation you’ve either loved or hated since Caitlyn Jenner showed up in lingerie.
Arts & Entertainment
Here’s everything queer that happened at the 97th Oscars
Let’s just say Cynthia Erivo and Arianna Grande blew us away so far into the sky with their performance, we defied gravity

First off, let’s congratulate the winners — and no, we are not including Emilia Peréz in the official winners category — though the cast and crew did snag a few ‘wins.’ The real winners were actors and actresses who graced the Red Carpet with dashing and smashing looks and those who stunned us with their acceptance speeches.
The Wizard of Oz intro to this year’s awards ceremony dazzled us all, as we were swept off our feet by Erivo and Grande’s dreamy and stunning Defying Gravity duet.
Let’s just say Cynthia Erivo and Arianna Grande blew us away so far into the sky with their performance, we defied gravity.
Erivo’s partner Lena Waithe, creator of TV series The Chi, also made an appearance from the audience during many moments sprinkled throughout the Oscars broadcast.
Though I’m sure Waithe looked at Erivo in awe and adoring admiration during her partner’s solo moment on stage, the way the cameras captured the adoring look Ari gave Erivo, just about melted our queer little hearts.
It seems like this year we saw alarmingly low BIPOC and LGBTQ+ representation overall in nominees and winners.
This is painfully surprising considering that we are peaking nearly 100 years of Oscars Awards ceremonies.
Still, the opening intro dazzled us all with Ari’s historically important Dorothy slippers clapping together in unison with the intro of the music.
Before getting into the winners, can I also just quickly mention how cringe it was for the acceptance song, for the Emilia Peréz Academy Award for Best Original Song? I hope I’m someday able to wipe that from my memory.
Okay, now that I got that off my chest, let’s get into the awards.
My biggest criticism about anyone at the Oscars this year is toward the Emilia Peréz cast and crew, whose silence spoke loudly when none of them thanked the trans community in any of their acceptance speeches.
They won Academy Awards for a storyline about the trans community and about the Mexican history of desaparecidos, but they did not acknowledge the community or the culture. Instead, I was expecting a shepherd’s cane to pull Camille Ducol backstage and off the mic.
In my humble opinion, this film is not getting nearly enough criticism as it should be getting for being called a Mexican film — yet not starring a single Mexican actor. The film also just about the worst musical numbers I have ever heard. Zoe Saldaña won the Oscar for Best Supporting Actress, for her role as a singing lawyer who helps the cartel leader played by Karla Sofía Gascón, undergo gender-affirming care and begin the process of transitioning.
The film featured a terribly choppy syntax not normally used in Spanish language, as well as accents and pronunciation that completely butchered the melody behind what maybe could have otherwise been somewhat palatable songs.
I’m just going to say it one more time for those in the back — we could have done without that embarrassing sing-along for one of the few wins Emilia Peréz snagged.
Many people across social media channels have tuned in to give their two cents on Emília Peréz. Most are calling for more disapproval of the film — and we couldn’t agree more.
And no, we’re not even going to waste precious time going over every single controversy currently plaguing the Emília Peréz cast and crew. There just isn’t enough time.
At the 97th Oscars ceremony, Paul Tazewell became the first out gay, Black man to win the Oscar for Best Costume Design for his work on the box-office hit, Wicked. In my humble opinion, it was a well-deserved win, but it’s also safe to say that it was tough competition as the other nominees designed the costumes for The Complete Unknown, Conclave, Gladiator II and Nosferatu.
Paul Tazewell, the celebrated costume designer who is renowned across Broadway, regional theatres and the big screen got his second nomination and his first win for his work and we are just over-the-moon about it. Wicked also took home the award for Best Production Design. Production designer Nathan Crowley and set decorator Lee Sandales, accepted the award and in Sandales’ acceptance speech, he thanked his husband.
Queen Latifah made a grand appearance and stunned the audience with her tribute to the late Quincy Jones, who passed away in November and who left behind an immense legacy in the music industry.
All in all, only two queer nominees took home awards.
Now, let’s get into Conan’s non-funny jokes.
This isn’t necessarily a queer recap moment, but we as we queers at LA Blade, did have some queer thoughts about this issue. Conan hosted the 97th Academy Awards and we’re going to make a guestimation that 97 percent of his jokes did not hit.
I think most of us were definitely expecting a joke or two about Garcón, but the two that Conan delivered, were at best mediocre. “Anora uses the F word 479 times, that’s only three more than the record set by Karla Sofía Gascón’s publicist,” said Conan on stage. “And if you are going to tweet about the Oscars, remember, my name is Jimmy Kimmel.”
At this point, I’m not even sure if it was really the audience laughing, or if it was some sort of button that plays 90s canned laughter when pressed by the show producers when the jokes aren’t funny and no one is actually laughing.
So, who slayed with their fits and who didn’t at the Red Carpet and afterparty?
It’s safe to say that Colman Domingo, Erivo and Grande were among the best dressed at this year’s Oscars at the Dolby Theatre in Hollywood. Every single one of their looks, ATE.
What were some of your favorite looks? What were others who didn’t deliver?

‘The Broadway Cage Match’ ready to rumble at WeHo’s Musical Mondays

Over 36,000 Angelenos unite for ‘Fighting the Oligarchy’ rally

New mayor Chelsea Byers, hopes to make WeHo a model city for others to follow

EXCLUSIVE: Garcia demands answers on deportation of gay Venezuelan asylum seeker

US lists transgender Brazilian congresswoman’s gender as ‘male’ on visa

Musical Mondays, a mainstay in WeHo nightlife, celebrates 16 years

Discredited former cop played ‘key role’ in deportation of gay make-up artist

A Night of legacy, love, and liberation: Inside the 2025 April Fool’s Ball

‘Bring it to Brunch’ returns to West Hollywood

LGBTQ+ advocacy group joins Myanmar earthquake relief effort
-
 a&e features5 days ago
a&e features5 days agoMusical Mondays, a mainstay in WeHo nightlife, celebrates 16 years
-
 National3 days ago
National3 days agoDiscredited former cop played ‘key role’ in deportation of gay make-up artist
-
 Arts & Entertainment2 days ago
Arts & Entertainment2 days agoA Night of legacy, love, and liberation: Inside the 2025 April Fool’s Ball
-
 Arts & Entertainment4 days ago
Arts & Entertainment4 days ago‘Bring it to Brunch’ returns to West Hollywood
-
 Myanmar4 days ago
Myanmar4 days agoLGBTQ+ advocacy group joins Myanmar earthquake relief effort
-

 a&e features4 days ago
a&e features4 days agoPeppermint thrives in the spotlight
-

 California3 days ago
California3 days agoSouth Park provides green space to a predominantly Latino community
-

 Arts & Entertainment2 days ago
Arts & Entertainment2 days agoSouth Coast Repertory Theatre hosting world premiere production
-

 Movies2 days ago
Movies2 days agoHeartfelt ‘Wedding Banquet’ remake a romcom worth seeing
-
 Brazil1 day ago
Brazil1 day agoUS lists transgender Brazilian congresswoman’s gender as ‘male’ on visa